


 Sign Out
Sign Out

Children: 0.5-1 mg twice daily.
Maintenance: The maintenance dose should be individualised and should be the lowest dose, which keeps the patient symptom-free. Recommended doses are: Adults: 0.5-1 mg twice daily.
Children: 0.25-0.5 mg twice daily.
Dosage in exacerbations of COPD: Patients should be treated with daily doses of 4 to 8 mg of 'PULMICORT RESPULES', divided into two to four administrations, until clinical improvement is achieved, but for no longer than 10 days.
The use of nebulised budesonide has not been evaluated in clinical trials in patients with an exacerbations of COPD with respiratory failure requiring invasive mechanical ventilation or admission to intensive care unit.
Time to effect in exacerbations of COPD: Following inhaled administration of 'PULMICORT RESPULES' for the treatment of exacerbations of COPD the time to symptom improvement is comparable to administration of systemic corticosteroids.
Acute laryngotracheobronchitis (CROUP): In infants and children with croup the usual dose is 2 mg of nebulised budesonide given as a single administration of 'PULMICORT RESPULES'.
MODE OF ADMINISTRATION: 'PULMICORT RESPULES' should be administered from a suitable nebuliser. The dose delivered to the patient varies between 40-60% of the nominal dose depending on the nebulising equipment used. The nebulisation time and the dose delivered is dependent on flow rate, volume of nebuliser chamber and volume fill. A suitable fill for most nebulisers is 2-4 mL.
Some sedimentation may occur during storage of 'PULMICORT RESPULES'. If this does not readily resuspend completely upon shaking, the 'RESPULE' should be discarded.
Dose division and miscibility: Pulmicort Nebuliser Suspension can be mixed with 0.9% saline and with solutions for nebulisation of terbutaline, salbutamol, fenoterol, acetylcysteine, sodium cromoglycate or ipratropium.
The admixture should be used within 30 minutes.
Single dose units can be divided, to allow dose adjustment. The single dose unit is marked with a line (Pulmicort 0.25 mg/ml and 0.5 mg/ml only). This line indicates the 1 ml volume when the single dose unit is held up-side down. If only 1 ml is to be used, empty the contents until the surface of the liquid reaches the indicator line. Store the opened single dose unit in the envelope, protected from light. Opened single dose units should be used within 12 hours.
Please note that if only 1 ml is used the remaining volume is not sterile. (See table.)
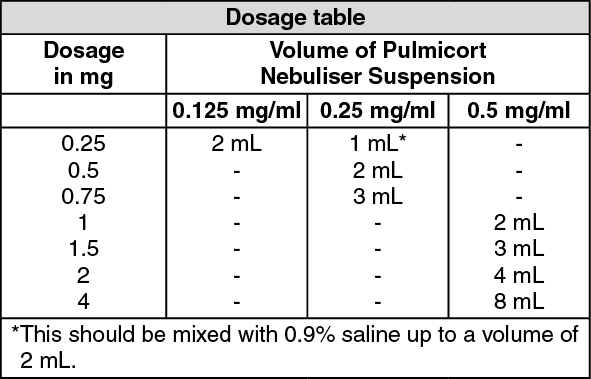 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePatient Instructions: 1. It is essential that the patient be instructed that 'PULMICORT' is a preventative agent, which must be taken regularly and is not to be used as sole therapy to relieve an acute asthma attack.
2. The patient should be instructed in the proper use of the inhaler device considered appropriate for his/her particular needs. A full set of instructions are provided with each pack of 'PULMICORT'.
Improvement in asthma control following inhaled administration of Pulmicort Nebuliser Suspension can occur within 3 days of initiation of treatment, although maximum benefit may not be achieved for 2-4 weeks.
Patients - maintained on oral glucocorticosteroids: Pulmicort Nebuliser Suspension may permit replacement or significant reduction in dosage of oral glucocorticosteroids with maintained or improved asthma control.
Initially, Pulmicort Nebuliser Suspension should be used concurrently with the patient's usual maintenance dose of oral glucocorticosteroid. After approximately one week the oral dose is gradually reduced to the lowest possible level. A slow rate of withdrawal is strongly recommended. In many cases it is possible to completely substitute the oral glucocorticosteroid with Pulmicort Nebuliser Suspension.
During withdrawal, some patients may experience symptoms of systemic corticosteroid withdrawal, eg, joint and/or muscular pain, lassitude and depression, despite maintenance or even improvement in pulmonary function. Such patients should be encouraged to continue with Pulmicort Nebuliser Suspension but should be monitored for objective signs of adrenal insufficiency. If evidence of adrenal insufficiency occurs, the systemic corticosteroid doses should be increased temporarily and thereafter withdrawal should be continued more slowly. During periods of stress or during a severe asthma attack, transfer patients may require supplementary treatment with systemic corticosteroids.